


CASES OF THE WEEK - “Bleeding Meckles Diverticulum (Three Short Cases)” by Dr Shekhar Shikare, Consultant & HOD, Nuclear Medicine, NMC Royal Hospital Sharjah
Meckel's diverticulum is the most common congenital anomaly of the gastrointestinal tract involving the small bowel and terminal ileum. Meckle's diverticulum is a remnant of the omphalomesentric duct /vitelline duct and is an abnormal pouch or sac opening from the small intestine. Most of the lesions remain asymptomatic throughout life, however complications may arise including hemorrhage, intussusception, volvulus and diverticulitis. In children, rectal bleeding is the most common complications while obstruction in the form of volvulus and intussusception is the most common presentation in adults.
Procedure-The Meckel's scan involves planar, scintigraphy detection of Tc-99m pertechnetate, an anion which is intravenously infused and selectively taken up by mucous secreting cells lining gastric and ectopic gastric mucosa. Visualization is improved by pretreatment with cimetidine /pant gastrin/glucagon.
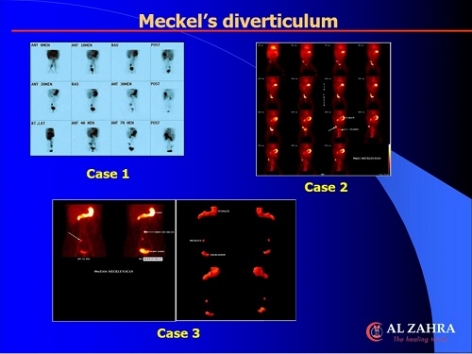
Case 1
4 years old boy with history of bleeding per rectum.
99mTc Pertechnetate Mackles Scan shows focal area of abnormal tracer accumulation in right iliac fossa region.
Surgery-Meckel’s
Case 2
24 years old male with h/o passing maroon colored stool for 6-7 days. Gastroscopy-Normal, Colonoscopy-full of blood.
99mTc Pertechnetate Mackles Scan shows focal area of abnormal tracer accumulation in right iliac fossa region (as shown with arrows).
Surgery-Meckel’s
Case 3
8-month-old child with three episodes of Malena.
99mTc Pertechnetate Mackles Scan shows focal area of abnormal tracer accumulation in right iliac fossa region more laterally(as shown with arrows).
Surgery- Meckel’s.
Ectopic mucosa is present in ∼50%, of which 60% contain gastric mucosa, which increases to 90% of bleeding Meckel's diverticula. Diagnostic accuracy of the Meckel's scan is >90% in the pediatric population but is less accurate in adults (sensitivity 62.5%, positive predictive value 60%, which is in part because complications in adults are less commonly associated with ectopic gastric mucosa. This data indicates that based on the clinical suspicion, diagnosing Meckel's diverticulum should be pursued as a cause of obscure GI bleeding and may require a multi-modality diagnostic approach.
Meckel's diverticula that contain gastric mucosa are capable of concentrating 99m-Tc-pertechnetate. Therefore, if a diverticulum is discovered and removed during surgery that was not detected by Meckel's scintigraphy, chances are that it contained some other type of tissue such as pancreatic, duodenal or colonic mucosa. False negative studies can be caused by diverticula that contain mucosa other than that of gastric origin or necrosis of the ectopic gastric tissue.
In a negative scan, the CT images can help to identify other causes of abdominal pain and bleeding. Meckel's scan along with SPECT/CT co-registered imaging should always be considered to optimize the diagnosis of cause of GI bleed, abdominal pain, and localization of Meckel's diverticulum.