


CASE OF THE WEEK – “HYPERTROPHIC OSTEOARTHOPATHY ON BONE SCINTIGRAPHY & THE ROLE OF HYBRID SPECT CT IMAGING” by Dr. Shekhar Shikare, HOD & Consultant, Nuclear Medicine at NMC Royal Hospital Sharjah
Case report
67 years old lady with history left leg pain since last 5 to 6 weeks related to day-to-day activities within the house. Also, on & off severe pain in left leg laterally during the sleep and while getting up.
Pain in both the knees related to walking & restricted joint movements since last six months.
Suspected to have popliteal nerve syndrome /tendinitis
X-rays left femur/ tibia-Diffuse sclerosis involving the visualized shaft of femur up to distal meta diaphyseal junction. X-rays right side shows similar density in femur shaft.
MRI of the left femur
Non contrast MRI finding of left femur reveals, near circumferential low to intermediated cortical thickening with heterogeneous marrow involving entire visualizes diaphysis of left femur. Screening right femur shows symmetrical thickening with heterogeneous diaphyseal marrow. Bilateral symmetrical thickening with heterogeneous diaphyseal marrow suggesting non-aggressive osseous lesion. The possibility of metabolic etiology/hypertrophic osteodystrophy, however metastasis needs to be ruled out
MRI left knee joint
Unsharp villous contours with thinning of cartilage and hyperintensities of the cartilage with fissuring seen on medial and lateral aspect of patella with underlying bone marrow edema at lateral facet of patella suggestive of chondromalacia patella grade IV. Hyperintensity seen in prepatellar soft tissue extending along the patellar tendon anteriorly suggestive of prepatellar bursitis. Interstitial edema in anterior cruciate ligament. No ligamentous tear. Grade I hyperintensity seen involving posterior horn of medial meniscus.
Biochemical parameters
TSH 2.1 mIU/ml, Glycated hemoglobin 6.0% (normal (<5.7), Lipid profile- Abnormal, Urea in serum 50.50 mg/dl (17.12-49.22), Sr creatinine 0.67 mg/dl (0.51- 0.95), Sr Uric acid 6.30 mg/dl (3.5- 7.30), Sr alkaline phosphatase 101.00 U/L (47.0-119.0), Sr calcium 9.6 mg/dl (8.60-10.30), Sr Zinc 55.70 microg/dl (60.10-120.30), Sr Iron 37.0 (33.0-193.0), Vit D 50.8 ng/ml (<30 deficient), Sr ferritin 141.0 (4.63-202.0) Urine analysis-negative. CBC- hemoglobin 12.4 gm/dl, RBC 4.51, and WBC are in normal range.
99mTc-MDP Bone Scintigraphy (Whole Body & Hybrid SPECT CT)
FINDINGS
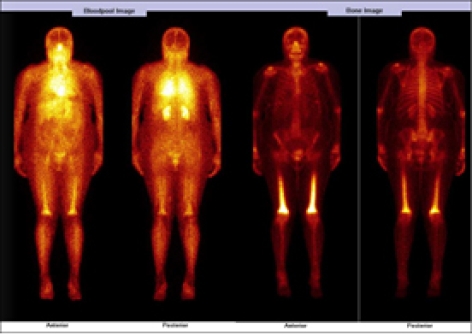
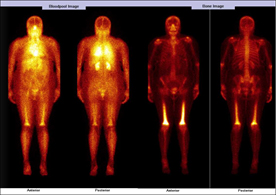
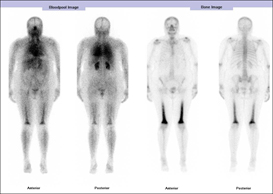
WHOLE BODY BLOOD POOL IMAGES
Symmetrical abnormal pooling of tracer seen involving lower 2/3rd of both the femur bones.
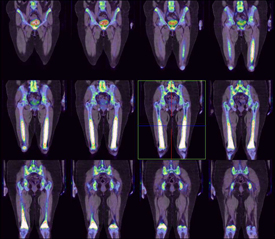
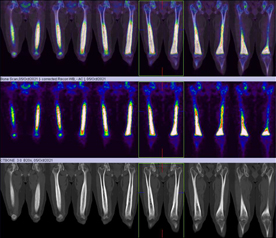
WHOLE BODY BONE & HYBRID SPECT CT IMAGES OF PELVIS TO KNEES
It shows abnormally increased tracer uptakes in
Symmetrical increased tracer uptakes seen involving lower 2/3rd of both the femur bone (anterior>posterior).
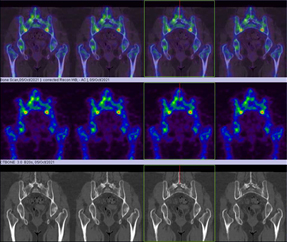
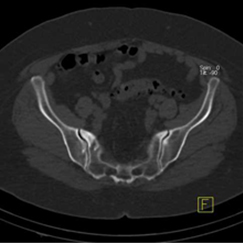
The S.I. joint inferiorly.
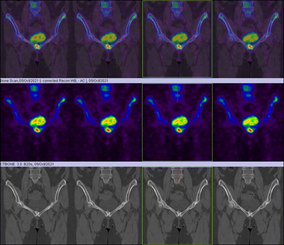
Symphysis pubis
Left ischial bone inferio-laterally.
Bilateral wrist and hand joints? due to OA.
Rest of the skeletal show’s normal tracer uptake pattern.
IN VIEW OF HYBRID SPECT CT FINDINGS
THE BILATERAL SYMMETRICAL LOWER 2/3RD FEMUR BONE ABNORMALITY IS LIKLEY TO BE DUE TO HYPERTROPHIC OSTEOARTHOPATHY (figure 1,2,3,4, 5 & 6)
THE BILATERAL S.I. JOINT ABNORMALITY COULD BE DEGENERATIVE (figure 5)
THE SYMPHYSIS PUBIS ABNORMALITY COULD BE DEGENERATIVE (figure 6)
THE LEFT ISCHEAL BONE ABNORMALITY MOST LIKELY TO BE DUE TO AVULSION INJURY (figure 7)





Discussion
Hypertrophic osteoarthropathy (HOA) is a syndrome characterized by clubbing of the digits, periostitis of the long (tubular) bones, and arthritis can be primary (hereditary or idiopathic) or secondary. Secondary HOA, which accounts for about 80% of HOA cases, is associated with an underlying pulmonary, cardiac, hepatic, or intestinal disease and often has a more rapid course. As a paraneoplastic syndrome, it most commonly occurs with pleural or pulmonary tumors; however, other tumors (eg, nasopharyngeal carcinoma and esophageal cancer) may also be involved.
Bone scintigraphy typically demonstrates a symmetric linear increase in tracer accumulation along the diaphyseal and metaphyseal surfaces of long bones (the railroad-track pattern). In addition to being used for diagnosis, bone scintigraphy can be used to evaluate the response to therapy, as scintigraphy findings can resolve after treatment of the underlying secondary cause.
Teaching point
99mTc-methylene diphosphonate bone scintigraphy (Whole body & Hybrid SPECT CT) is a sensitive method to detect hypertrophic osteoarthropathy and provides both the anatomical and functional information.