Glue Ear in Children

What is glue ear?
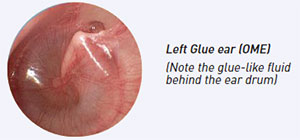
Most parents will have heard the term ‘Glue ear’, which is the common name for a medical condition known as Otitis Media with Effusion (OME). The disorder arises from dysfunction of the natural tube, called Eustachian tube, which connects the ear to the back of the nose. This results in the accumulation of fluid behind the ear drum and consequently hearing loss. Family history is a major risk factor for OME. Glue ear is not an infection or a painful condition, in fact, it is a silent disorder. Most children will have fluid behind the eardrums at some stage before age 11, but it usually resolves spontaneously in the majority of cases without any adverse effect. However, in some children the fluid persists and results in multiple problems related to reduced hearing, education and behaviour.
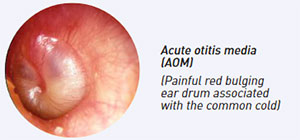
Glue ear should not be confused with the painful red bulging ear drum (acute otitis media, AOM) associated with runny nose, fever and the upset child.
What are the problems associated with glue ear?
There is strong research evidence to show that cases of persistent bilateral glue ear can result in hearing loss which in turn leads to poor speech and language development. In addition, a history of persistent untreated glue ear is associated with a lower intelligent quotient (IQ) score, reduced reading ability and behavioural problems such as anti-social behaviour involving the law, hyperactivity, social immaturity and leaving school without qualifications.
How is glue ear treated?
A UK study (known as TARGET Trial) revealed that a period of watchful waiting for at least 3 months is beneficial as the condition may resolve spontaneously. Medicines such as antibiotics, antihistamines or decongestants are not helpful, unless there are co-existing signs of infection or allergy.
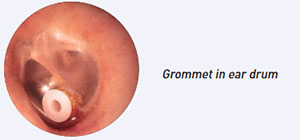
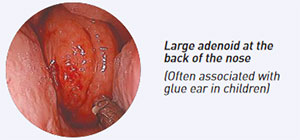
Alternative therapies like homeopathy, cranial osteopathy, acupuncture massage and probiotics do not work. Insertions of ventilation tubes (grommets) into the ear drums have been shown to be effective, but the beneficial effect fades after 6 months. Grommets in combination with adenoidectomy (surgical removal of the adenoid at the back of the nose) prolong the overall benefits at 6-18 months. The two procedures are complementary and cost effective, especially in children with frequent upper respiratory tract infections. The majority of cases of chronic glue ear (greater than 3 months) are treated primarily with grommets and adenoidectomy, except in special cases such as Down syndrome where hearing aids are recommended. In normal children, hearing aids may also be used when surgery is contraindicated or not acceptable.