


CASES OF THE WEEK – “Osteoid osteoma - The role of gamma probe guided osteoid osteoma surgical removal” by Dr ShekharShikare, Consultant & HOD, Nuclear Medicine
OSTEOID OSTEOMA (SHORT CASES)
THE ROLE OF GAMMA PROBE GUIDED OSTEOID OSTEOMA SURGICAL REMOVAL (CURRENT SENARIO).
Osteoid osteoma is prevalent among children and young adults but can be found in older individuals. It is more common in men. Osteoid osteomas have been described in virtually all bones (except in sternum) and are more frequent in long bones, especially in the proximal femur. The diagnosis of osteoid osteoma is based on clinical, radiographic, and scintigraphy findings. Frequently, patients have pain for months or years until the lesion is discovered.
Bone scintigraphy is the best method for localization and diagnosis of the lesion. The classic scintigraphic appearance of a double density is very specific for osteoid-osteoma and is used as a guide for a dedicated computerized tomography (CT) study.
Initial treatment of osteoid osteoma is nonoperative. Surgical intervention is generally indicated for patients whose pain is unresponsive to medical therapy, those who cannot tolerate prolonged use of nonsteroidal anti-inflammatory drugs (NSAIDs), and those who are not amenable to activity restrictions.
Lesions in anatomically inaccessible areas, such as the femoral head and neck, result in considerable surgical morbidity, and their removal may cause complications or disability more severe than that associated with the original condition.Other disadvantages of surgical treatment include difficulties in identifying and localizing the nidus at the time of surgery, postoperative restriction of activity that may be required after bone is removed, and an awkward anatomic location of the tumor that may require an extensive surgical approach.
Localization of lesion
Preoperative
Regardless of the method of treatment, its success highly depends on preprocedural exact localization of the nidus / lesion is the most important determinant of successful operative removal.
Radionuclide scanning and computed tomography (CT) have been most helpful in localizing the tumor. Radionuclide scanning assists in the localization and diagnosis of osteoid osteoma in its early stages. It is also used in ruling out multicentric processes, which can occur in osteoid osteoma. On the other hand, CT can assist in preoperative localization, and it is useful in precise localization of the nidus in the hip or the spine.
Intraoperative
Various methods have been used for intraoperative localization and identification of osteoid osteomas to minimize bone resection and to help ensure complete excision of the tumor. Intraoperative scanning has evolved because of the excessively wide excision necessary in the past that had to be planned to help guarantee complete removal of the lesion. However, even with the use of frozen sections, adequate excision is not ensured.
Tetracycline fluorescence under ultraviolet (UV) light requires patients to take tetracycline before surgery (4 mg/kg body weight by mouth four times daily for 1-2 days). The difficulty of intraoperative identification of the nidus often leads to non-excision of the lesion. Information must therefore be obtained from the excised bone with pathologic examination. If the nidus is not in the specimen, further resection of the bone is required, resulting in unnecessary and excessive removal of bone.
Intraoperative radiography can be helpful in localizing the lesion in reference to a guide pin inserted into the bone. Multiplanar fluoroscopy can help in localizing the nidus if it is in cancellous bone, where sclerotic reactions are minimal. By comparison, cortical lesions contain reactive sclerosis that may obscure the nidus, leading to incomplete removal of the lesion and resulting in recurrence.
Intraoperative radioisotope scanning for osteoid osteoma, the advantages of this approach are that it employs a radionuclide scintillation probe (Gamma Probe) that is easy to use and reliable, it minimizes bone resection, and it does not prolong surgery. It can help the surgeon and pathologist confirm resection of the tumor and localize the lesion for histologic examination. Intraoperative radioisotope scanning is the only technique that aids in verifying complete surgical excision of the lesion (success rate, 94%). Furthermore, it keeps procedural morbidity at its lowest level. CT scan is helpful for precise localization of the nidus in the hip or spine. It is also helpful in precisely defining the location of the tumor and the extent of osseous involvement.
The most frequently performed surgical techniques are in-block resections and nidus curettage with or without adjuvant. Some institutions prefer percutaneous CT scan-guided thermal ablation of the nidus with a radiofrequency probe as the treatment of choice. However, this method should not be used in the vicinity of neurovascular structures. Except for percutaneous CT-scan-guided procedures, a major concern during open osteoid-osteoma operation is localization and resection of the nidus with minimal disruption of surrounding tissues to avoid complications.
FEW CASES OF OSTEOID OSTEOMA FOR ILLUSTRATION PURPOSE
Case 1
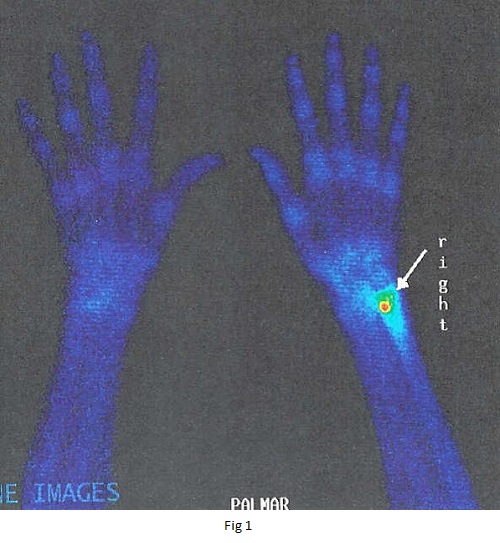
Right radius bone OSTEOID OSTEOMA distally with typical double density sign (fig 1)
Case 2
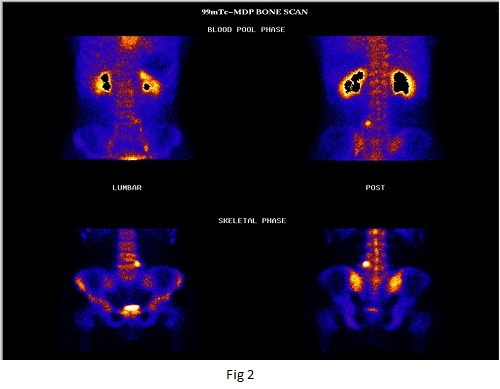
L5 vertebra OSTEOID OSTEOMA on the left side (ideal candidate for Gamma probe guided removal)- fig 2
Case 3
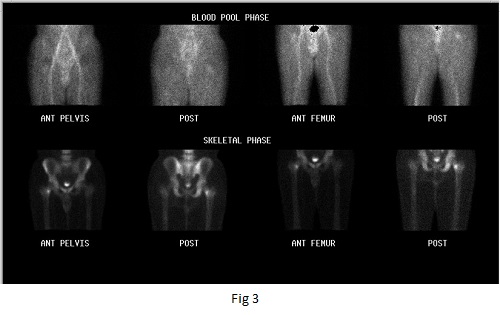
Left lesser trochanteric OSTEOID OSTEOMA (ideal candidate for Gamma probe guided removal)-fig 3
Case 4
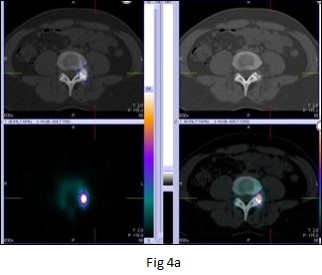
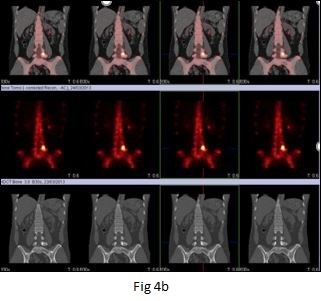
Operated case of Osteoid Osteoma (recurrence)
27 years old male with history of recurrent back pain History of excision of osteoid osteoma from the left pedicle of L5 vertebra.
MRI scan - suspicious of recurrence of osteoid osteoma left pedicle of L5 vertebra.
SPECT-CT BONE images-
Focally active abnormality in left L5 Pedicle favors recurrence (ideal candidate for Gamma probe guided removal)- fig 4a and b
Conclusion
Bone scintigraphy followed by intraoperative nidus detection with a hand-held gamma probe gives the surgeon precision when resecting osteoid osteoma. It is a good choice when the percutaneous radiofrequency ablation is not available or cannot be done.
The radiation exposure of bone scintigraphy compares however very favorably with that of CT. Additionally, by Probe guided surgery (PGS), use of the intraoperative X-ray is reduced since localization of the tumor is facilitated by the gamma probe.
Probe guided surgery (PGS) is still a good option when the tumor is difficult to localize or when RFA is not possible due to the proximity to neural structures.