


CASES OF THE WEEK – “Multi Systemic Inflammatory Syndrome in Children” by Dr Sanjiv Kakkar, Specialist Paediatrics
10 year old boy (Wt-69 kg; BMI-31.12 kg/m2) presented to the Hospital ER with the complaint of high grade intermittent fever and cough of 3 days duration. He had a history of exposure to a case of COVID -19(father).
Initial COVID-19 RT-PCR done outside the Hospital was negative.
He had been given Azithromycin and supportive medication from a clinic, but to no avail.
On examination at admission, the child had generalized fatigue, high fever (38 degrees) and cough. No rashes, icterus or petechiae . Systemic Examination revealed harsh vesicular breath sounds bilaterally in the lungs. No neurological deficit.
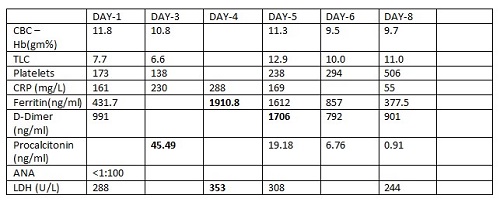
Investigations done showed high acute inflammatory markers.
He was initially started on IV antibiotics and supportive medication, and a diagnosis of Acute Bronchitis was kept in mind.
The child continued to have moderate grade intermittent fever. He also developed pain abdomen, vomiting and loose stools, and followed by bilateral conjunctivitis and sub conjunctival hemorrhage in the eyes.
Repeat investigations showed markedly elevated inflammatory markers . Hence , the antibiotics were upscaled .
An echocardiography done , was normal.
In view of the history of exposure to a case of COVID-19, multi-systemic involvement and progressive rise in the levels of inflammatory markers, a diagnosis of Multi Systemic Inflammatory Syndrome in Children(COVID-19) was entertained, and it was planned to give IVIG to the child @2gm/kg.
Thereafter, the child showed a gradual progressive improvement in his condition .The inflammatory markers also reduced.
The child stabilized , and was finally discharged home in a stable condition.
At this stage, it would be pertinent to revisit the definition of MIS-C as laid down by WHO
A case of MIS-C is one which meets the following criteria ( All 6 criteria must be met)
- Age: 0 to 19 years
- Fever for > 3 days
- Clinical signs of multisystem involvement( at least two of the following)
- (a) Rash, bilateral non – purulent conjunctivitis or mucocutaneous inflammation signs(oral , hand or feet)
- (b) Hypotension or shock
- (c) Cardiac dysfunction, pericarditis, valvulitis or coronary abnormalities(including echocardiographic findings or elevated troponin)
- (d) Evidence of coagulopathy ( prolonged PT or PTT; elevated D-dimer)
- (e) Acute gastrointestinal symptoms( diarrhea, vomiting or abdominal pain )
- Elevated markers of inflammation ( ESR, CRP or Procalcitonin)
- No other obvious microbial cause of inflammation
- Evidence of SARS – CoV-2 infection. Any of the following:
- (a) Positive SARS CoV-2 RT –PCR
- (b) Positive serology
- (c) Positive antigen test
- (d) Contact with an individual with COVID-19
MIS-C is a dangerous and potentially lethal condition.
In my view, the child being morbidly obese (BMI -31.12 kg/m2 ) was a major risk factor for the MIS-C. However, fortunately, he did not require ventilatory or vasopressor support, and made a quick recovery with prompt recognition and appropriate medical attention.