CASES OF THE WEEK - “Hepatobiliary scintigraphy (hbs) adjunt hbs spect- ct fused imaging in detection of active biliary leak and anatomical localisation of the site following post laproscopic cholectsectomy (unusual case of medical management)” by Dr ShekharShikare, Consultant & HOD, Nuclear Medicine, NMC Royal Hospital Sharjah
Gallstone disease is one of the most common digestive health problems.. Laparoscopic cholecystectomy (LC) is now the gold standard for gallbladder removal in the management of symptomatic cholelithiasis. Bile leak is a potential complication of this procedure and the cystic duct stump is the most common site of leakage. Early diagnosis and treatment of bile leak is crucial in decreasing the morbidity and mortality related to this complication.
Postsurgical bile leaks can be associated with significant morbidity and even mortality, if not identified and treated at an early phase. Hepatobiliary scintigraphy (HBS) scan is an important test for detection of bile leaks in the postoperative abdomen. However, the lack of anatomical details on planar images can make interpretation difficult, however correlation with SPECT/CT is very important.
We present a case of active bililary leak following laproscopic cholecystectomy. Hepatobiliary scintigraphy ( HBS) show presence of an active bile leak from the gall blader fossa region (cystic duct stump) and adjunct SPECT CT FUSED imaging showed the anatomical site of the leak.
Subsequently patient has been managed conservatively as the
distal end of the fusiform shaped bile leak collection sealed off automatically.
44 years old female presented with history of right upper quadrant pain on and off. Clinical assessment lead to suspicious of cholecystitis, Liver function tests-were normal in range, Coagulation profile were normal in range and, complete blood counts were normal in range.
Ultrasound of the abdomen-Hepatomegaly with fatty liver changes and gall bladder stones.
She underwent laproscopic cholecystectomy. Post operative ultrasound examination of abdomen-(1) Pocklet of fluid seen gall baldder fossa bed, perihepatic and pelvic collection. Post operative ultrasound examination of abdomen-(2), fluid pocket in the gall bladder bed which increased from 5.1*1.6 cc done on 25.6.17 to approximately 5.9*3.4 cc today. Fluid noted around the liver margin (peri-heptic i.e.12.2 cc), small fluid pockets were also note in both the iliac fossa.
99mTc –Hepatobiliary Scintigraphy (3)
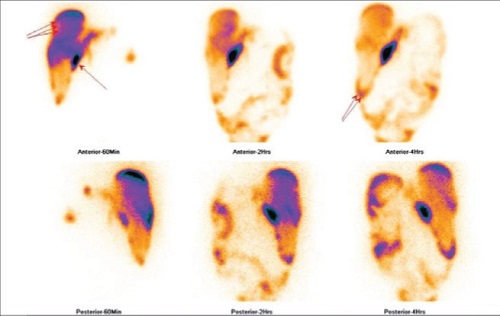
After intravenous administration of 99mTc-mebrofenin, sequential dynamic abdominal images were obtained over 60 min and static sequential images were obtained at 60 min,120 min and 4 hours respectively and SPECT-CT FUSED images at 60 minutes. It shows fairly good hepatocytic tracer extraction by the liver.Tracer excretion from the common bile duct route into
intestine is comparatively delayed and decreased but appears to be non obstructive and non dominant drainage pathway (approximately around 30% of drainage)
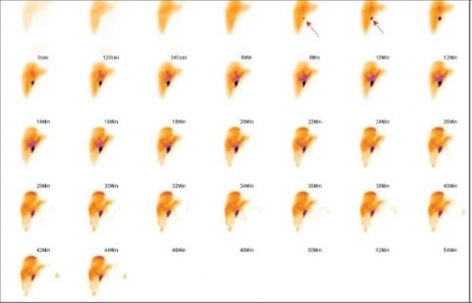
Abnormal tracer accumulation (leak) started seeing around eight minutes onwards in gall bladder fossa region, which kept on increasing in size and appearing like fusiform in shape and from the distal end of this fusiform shaped collection (figure 1 arrows), it has started moving downwards from the inferior border of the liver (approximately nineteen minutes onwards) and than towards the peri-hepatic region, right para-colic region and peritoneum and also seen in peri-spleenic region at four hours of images (figure 2) and it appears to be dominant drainage pathway ( approximatly around 70 % of drainage).
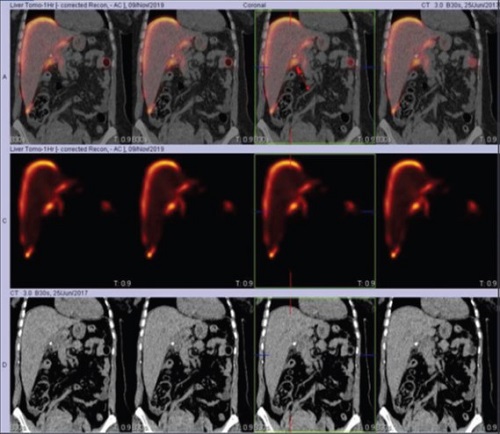
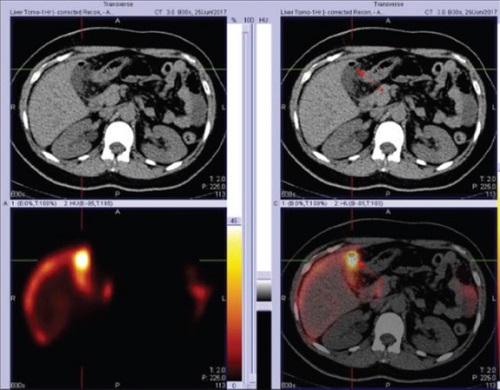
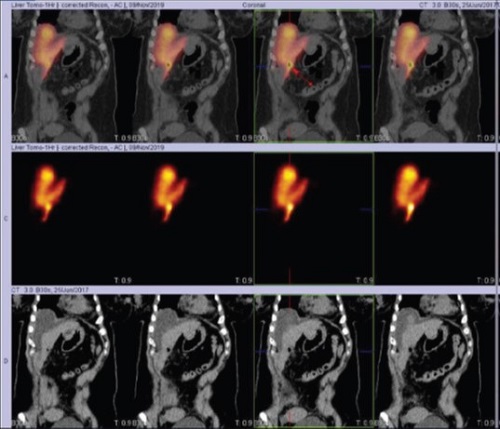
Adjunct SPECT/CT was performed at sixty minute selectively for precise anatomical localisation and it showed active site of the biliary leak from the gall bladder fossa region (fig 3) along with peri-hepatic tracer collection (fig 4,5 arrows). CT scan of abdomen with contrast (4)
Fluid still noted in the gall baldder bed. The periheptic and peri-spleenic collections have significantly reduced and are almost absent. Minimal fluid is seen at the base of right paracolic recess. This may represent a contained biliary leak with walled off collection. It may also contain serous fluid from the peritnoeal cavity and surgical packing used int procedure.
Based on the CT scan of abdomen with contrast findings, patient was been managed conservatively. Patient done clinically well and discharged home. This case demonstrates accurate localization of the site of bile leak through a direct sign, can be obtained with HBS and HBS SPECT/CT as shown in this case. The HBS SPECT/CT provides both anatomic and functional information and overcomes the lack of specificity of CT alone or detailed anatomic information of HBS alone.