


CASES OF THE WEEK - “Evaluation Of Leveen-shunt Patency Using Tc-99m Labelled Macroaggregated Albumin (Maa)” by Dr ShekharShikare, Consultant & HOD, Nuclear Medicine, NMC Royal Hospital Sharjah
CLINICAL APPLICATIONS OF NUCLEAR MEDICINE (EXCEPTIONAL GATROENTEROLOGY CASES)
EVALUATION OF LEVEEN-SHUNT PATENCY USING TC-99M LABELLED MACROAGGREGATED ALBUMIN (MAA).
Ascites is a common clinical finding with a wide range of causes. In approximately 10-15 percent of all these patients, it is refractory to first line treatment.1 Peritoneo-venous shunt (PVS) has been widely used as a suitable alternative to repeated large volume paracentesis especially for the treatment of patients with refractory ascites. Among the various complications associated with PVS, the most common one is the obstruction of the prosthesis, which occurs in 40-60 percent of patients during first year of follow-up. Evaluation of duct patency is very important in these patients presenting with gradually increasing abdominal girth after placement of Le Veen shunt tubing.
Here, we present a simple but very rarely performed technique of demonstrating PVS patency using Tc-99m labeled macro-aggregated albumin. The Le Veen peritoneo-venous shunt is designed to provide one way flow of sterile ascitic fluid from the abdomen to the vascular system.
Case
A 27 years old known cirrhotic female patient who underwent peritoneal venous shunting (PVS) 6 months ago, was referred for the evaluation of shunt.
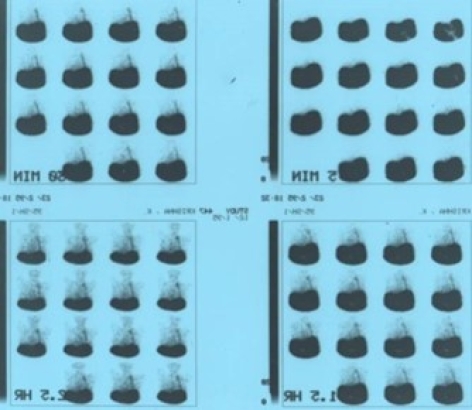
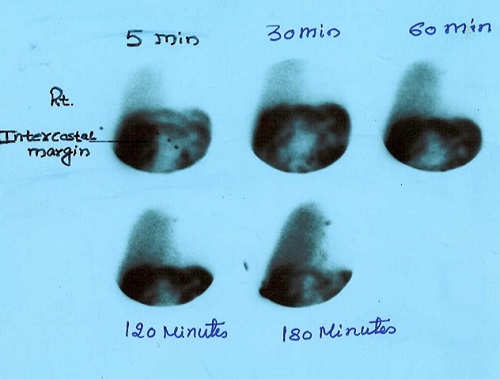
99mTc MAA Peritoneal Venous Shunting Shows Patency of the PV SHUNT
Hepatic hydrothorax refers to the presence of a pleural effusion (usually >500 mL) in a patient with cirrhosis who does not have other reasons to have a pleural effusion (examples cardiac, pulmonary, or pleural disease). Hepatic hydrothorax occurs in approximately 5 to 10 percent of patients with cirrhosis
Case
History of Cirrhosis of liver, ascites and right sided pleural effusion.
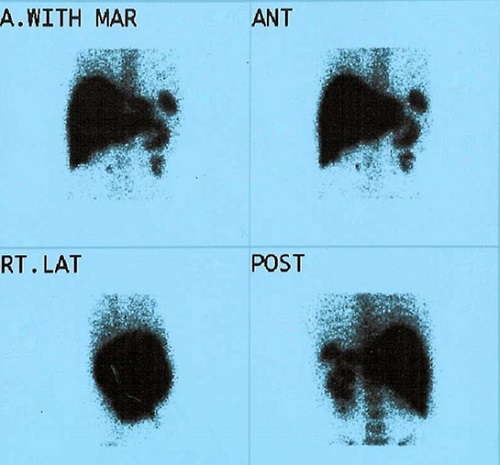
99mTc Sulphur Colloid scan showing diffusion of tracer on the right side of the lung (Hepatic hydrothorax).
Accessory spleen
It should be remembered that after resection of the proper spleen, accessory spleens may increase significantly, which enhances the risk of their being interpreted as metastases in radiological examinations or PET examinations.
The specificity of scintigraphy with sulphur colloid radiolabeled with Tc 99m in finding accessory spleens in patients after spleen resection is very high due to the absence of other parenchymal organs in the left upper abdomen, which would show radiotracer accumulation
Case
Suspected case of accessory Spleen with past history of Splenectomy.
99mTc Colloid scan showing accessory spleen
Role of Tc99m Sulphur colloid scintigraphy in differentiating non-cirrhotic portal fibrosis from cirrhosis liver
Cirrhosis is a consequence of chronic liver disease characterized by replacement of liver tissue by fibrosis, scar tissue and regenerative nodules leading to loss of liver function. Non-cirrhotic portal hypertension (NCPH) comprises a group of diseases that are characterized by an increase in portal pressure due to intra-hepatic or pre-hepatic lesions, in the absence of cirrhosis of the liver. It is not merely absence of cirrhosis, but also of hepatic venous outflow obstruction, such as veno-occlusive disease and Budd-Chiari syndrome.
Differentiation of NCPF and cirrhosis of liver is many times a clinical dilemma. The diagnosis of NCPF is established by the presence of features of PH like esophageal varices on endoscopy, raised splenic pulp pressure, collaterals on spleeno-porto-venography (SPV) or on ultrasound), by a definite exclusion of cirrhosis of the liver on clinical, biochemical, ultrasonography, surgical and histological findings and by exclusion of obstruction of spleno-portal axis on SPV and on Doppler ultrasound. Ultrasound findings that differentiated NCPF from cirrhosis included the absence of irregularities of intra-hepatic portal vein radicles, thickening of the portal vein wall ≥3 mm, a sudden narrowing of intra-hepatic second degree portal vein branches, and Gamna-Gandy bodies in the spleen and smooth surface of the liver. Liver biopsy is gold standard but it is invasive and a risky procedure in these patients with altered coagulation profile.
Tc99m Sulphur colloid has been used as an imaging agent for the liver and spleen. Subjective assessment of parameters such as the dimensions of the liver and spleen, colloid shift and uptake of radiopharmaceutical in the bone marrow have been used for both diagnosis of liver cirrhosis and evaluation of its progression. The distribution of radio-colloid uptake in the liver, spleen and bone marrow has been shown to correlate well with the severity of chronic liver disease, the severity of histological fibrosis, prognosis and hepatic function.
Relative distribution of radioactive colloid in cirrhotic livers using planar and SPECT techniques have shown that the Kupffer cell mass determined by the degree of relative hepatic and splenic uptake of colloid particles by the cells of the reticuloendothelial system correlates with disease severity and hepatic function in liver cirrhosis. They also implied that radioactive colloid distribution is a better estimate of disease severity than invasive tests. Thus, the uptake of radioactive colloid by the liver could be used to evaluate cirrhosis. Spleen volume undergoes modifications during the course of chronic liver disease. Measurement of spleen size and individual uptake of radio colloid by the spleen could be useful in evaluating spleen hyper function in patients with cirrhosis.
As per the literature colloid shift to the bone marrow (84 % vs. 7%), and decreased liver uptake (59% vs. 20%), was seen more often in cirrhotic group. Increased spleen size (100% vs. 67%) with no evidence of colloid shift to the bone marrow (84% vs. 7%), was more suggestive of NCPF. Increased bone marrow activity has been described in 16.6, 44. and 72.72% patients with Child A, B and C cirrhosis respectively. Normally approximately 85% of the colloid is trapped in the kuffer cells in the liver and remainder goes mostly to spleen and bone marrow. Distinguishing pattern in cirrhosis is explained by cirrhotic liver’s decreased extraction efficiency for the blood-laden colloid due to pH, extra- and intra-hepatic arterio-venous shunt and replacement of the liver parenchyma and sinusoidal kuffer cells by fatty infiltration, necrosis and fibrosis. Thus colloid not extracted by the diseased liver recirculates through the bone marrow and spleen and is engulfed by reticuloendothelial cells of these areas, resulting in significant uptake in the bone and spleen.
In conclusion 99mTc Sulphur colloid liver scan is a non-invasive procedure having a useful adjunctive role in clinical differentiation of cirrhosis from NCPF.
CASE
Budd-Chiari syndrome is a manifestation of hepatic outflow
obstruction which usually occurs at the level of inferior vena cava (IVC), hepatic veins and possibly at venule level. When some, but not all liver veins were occluded, markedly diminished uptake over the affected segments was usually seen (absence of uptake may occur in acute infarction and in chronic cases). When all major liver veins are occluded, markedly diminished uptake is seen over the peripheral parts of the right and left lobes with a triangular midline area excessive activity. The latter effect is probably caused by uptake in segments surrounding the inferior vena cava (frequently the caudate lobe) that have direct venous drainage. This liver-scan appearance is characteristic enough to warrant consideration of the Budd-Chiari syndrome as the first diagnosis.
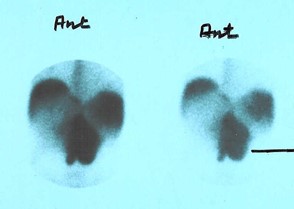
Figure 1 99mTc Sulphur colloid scan showing large sized caudate lobe with increased uptakes, while rest of the liver shows poor colloid uptakes (except in portion of right lobe with adequate uptakes (Budd-Chiari syndrome as shown with single line).
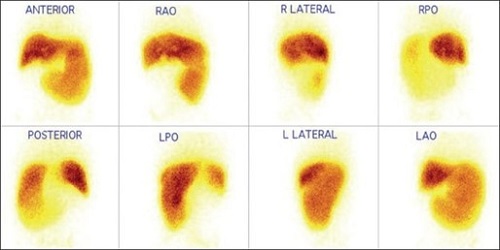
Figure 2 Tc99m sulfur colloid scan in case of NCPF showing adequate colloid uptake in liver with increased size and uptake in the spleen and no evidence of colloid shift to the bone marrow.
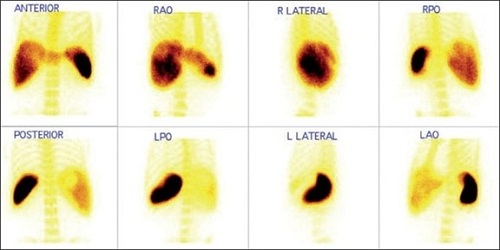
Figure 3 Tc99m sulfur colloid scan in case of cirrhosis of the liver showing impaired colloid uptake in the liver and increased uptake in the spleen with significant colloid shift to bone marrow
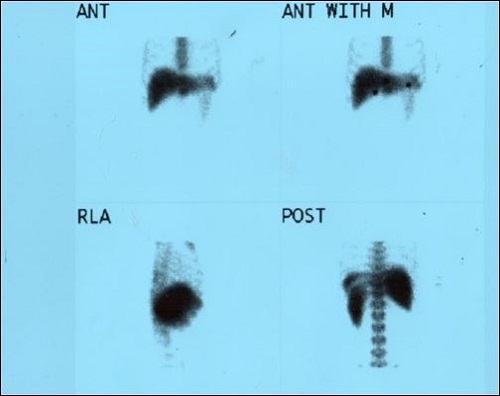
Figure 4 Tc99m sulfur colloid scan in case of cirrhosis of the liver showing impaired colloid uptake in the liver (but preserved functions) and increased uptake in the spleen with significant colloid shift to bone marrow
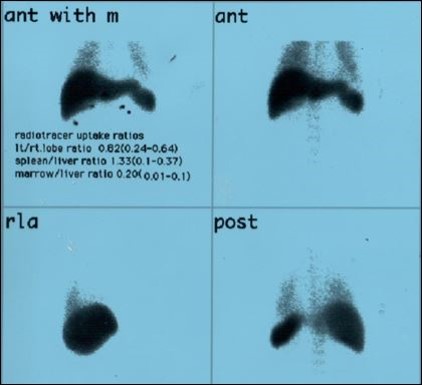
Figure 5 Tc99m sulfur colloid scan in case of cirrhosis of the liver showing impaired colloid uptake in the liver (but preserved functions) and increased uptake in the spleen with significant colloid shift to bone marrow and lung uptakes with quantitative parameters to see the severity of the liver disease.
Choledochal Cyst
A congenital anatomic malformation of a bile duct, including cystic dilatation of the extrahepatic bile duct or the large intrahepatic bile duct. Classification is based on the site and type of dilatation.
Much about the etiology, pathophysiology, natural course and optimal treatment of cystic disease of the biliary tree remains under debate. Gastroenterologists, surgeons and radiologists alike still strive to optimize their roles in the management of choledochal cysts. To that end, much has been written about this disease entity, and the purpose of this 3-part review is to organize the available literature and present the various theories currently argued by the experts. In part 2, we explore the details surrounding diagnosis, describing the presentation and imaging of the disease.
Technetium-99 HIDA scans are useful in the neonatal period to differentiate congenital CCs from biliary atresia, as the ultrasound images in both diseases are similar. Computed tomography and MRI are useful modalities to diagnose and determine the extent of intra-hepatic disease, such as type-IV A and type-V cysts. Once CCs have been diagnosed, careful treatment decisions need to be made. The third and final installation of this review series describes the management of biliary cystic disease.
Case
6 years old child with history of recurrent pain in abdomen.
USG suspected dilated CBD.
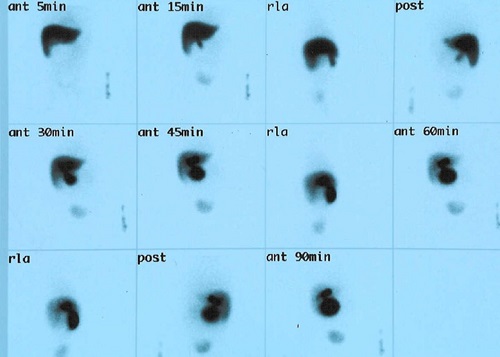
Figure 1 - 99mTc HIDA scan shows LARGE CHOLEDOCHAL CYST
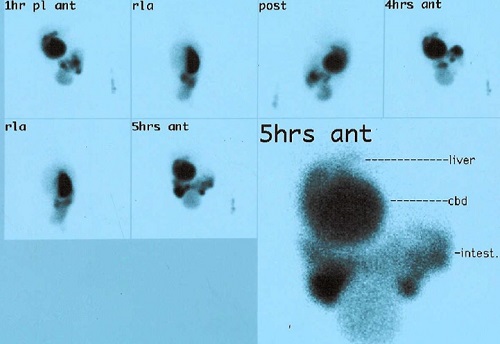
Figure 2 - 99mTc HIDA scan shows large choledochal cyst