


CASES OF THE WEEK – “A Pediatric Case of Meckel Diverticulum with uncommon presentation showing no lower Gastrointestinal Bleeding” by Dr ShekharShikare, Consultant & HOD, Nuclear Medicine
A Pediatric Case of Mecke Diverticulum with uncommon presentation showing no lower Gastrointestinal Bleeding
Meckel diverticulitis
Meckel diverticulitis is the inflammation of Meckel diverticulum, which is the most common congenital structural abnormality of the gastrointestinal tract. Despite this, it is an uncommon cause of acute abdomen and is often not correctly diagnosed pre-operatively.
Meckel diverticulum is seen in approximately 2% of the adult population and among those with symptoms, males are disproportionately affected compared to females in a ratio of 2-4:1 Meckel’s diverticulum (MD), the most common congenital anomaly of the gastrointestinal tract, has been described as the remnant of the omphalomesenteric duct. According to the rule of 2s, MD occurs in 2% of the population, with a male to female ratio of 2:1, is located 2 feet proximal to the ileocecal valve, the symptoms present ≤ 2.0 years, and it is approximately 2 inches long.
The prevalence of MD depends on the population studied. It increases, in descending order, in children with major malformation of the umbilicus, alimentary tract, nervous system, or cardiovascular system.
Meckel’s diverticulum is often clinically silent, particularly in adults, and the symptomatic picture may be abdominal pain, bowel obstruction or gastrointestinal bleeding. We describe the case a three-old child who presented with intestinal volvulus of the MD, an uncommon phenomenon in children of this age.
Case
A three-year-old child admitted with abdominal pain and vomiting since last two days.
On abdominal examination, pain was in the periumbilical area, but the abdomen was soft without tenderness and organomegaly. No masses were felt, and the bowel sounds were normal.
The biochemical measurement showed leukocytosis with neutrophilia. The rest of the laboratory data were within the normal limits.
Differential diagnosis was Meckel’s diverticulum /Enteric duplication cyst.
Refereed for 99mTc Pertechnetate Meckel’s Diverticulum scan
99mTc Pertechnetate Meckel’s Diverticulum scan
Dynamic 30 minutes & static 30 minutes abdominal images (figures 1,2,3) shows focal area of abnormal tracer accumulation in peri-umbilical region favoring presence of Meckel’s diverticulum (NON-BLEEDING TYPE).
Subsequently underwent laparoscopic surgical removal of the Meckel’s diverticulum.
Histopathological examination of the specimen confirmed Meckel’s diverticulitis.
Discussion
Although most MD is asymptomatic, if complications such as hemorrhage, perforation, intestinal obstruction, and diverticulitis occur, symptoms can appear in patients with MD. More than half of the patients who develop symptoms are aged ≤2 years.5
Meckel’s diverticulum often presents with hemorrhage or painless intestinal bleeding in children, in contrast to the symptoms of small bowel obstruction in adults.6 MD is the most common reason for massive lower gastrointestinal tract bleeding that is painless in children, or for massive melena, leading to shock.7 However, it should be born in mind that the presentation of MD is non-specific and can be variable.6
An intestinal obstruction relating to MD in children can result from intussusception, volvulus, diverticulitis, and Littre hernia. Of these, intussusception with MD as the leading point, followed by a mechanical volvulus of the small intestine around a persistent band that has attached the MD to the umbilicus are the most common.
Younger children with symptomatic MD are more susceptible to presenting with obstructive symptoms. The pediatric population in whom there is obstruction may display irritability, abdominal distension, abdominal pain, anorexia, nausea, and vomiting.
Half of MD-associated intussusception occurs in patients aged ≥3 years.7 Volvulus results when the small intestine twists around a fibrous cord, or Meckel’s band, tethering the MD to the umbilicus. It was shown in a case series study on 34 children with MD that the most common chief complaint was lower gastrointestinal bleeding (35.3%), abdominal pain (32.4%), vomiting (8.9%), and abdominal distension (2.9%) The most common MD symptoms in children in the study by Lee et al.10 were lower gastrointestinal bleeding (47.0%) and intestinal obstruction (32.4%). Our case is uncommon because the child first presented with upper gastrointestinal bleeding, as opposed to the more usual lower gastrointestinal bleeding, followed by bowel obstruction.
Neither intestinal obstruction nor volvulus due to MD are common features in children aged ≥2 years. In addition, the reports on pediatric cases of intestinal volvulus due to MD are few in number.
CONCLUSION
Meckel’s diverticulum should be considered in the differential diagnosis of acute abdominal pain and the signs and symptoms of bowel obstruction.
A Pediatric Case of Meckel Diverticulum with uncommon presentation showing no lower Gastrointestinal Bleeding
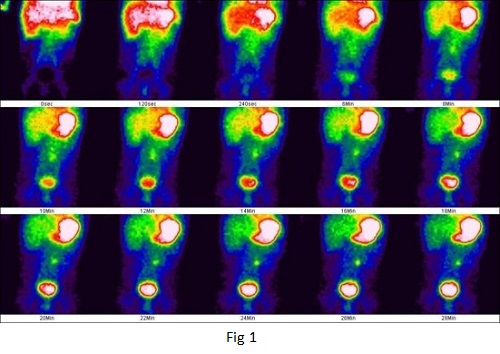
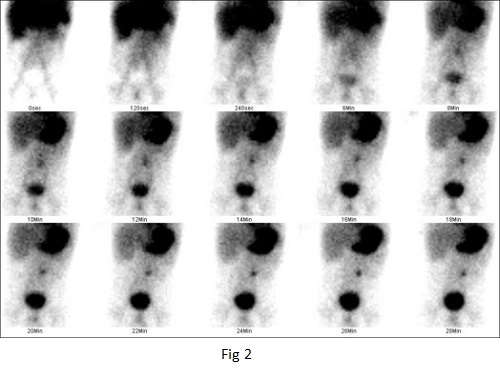
Figure 1,2 - 99mTc pertechnetate meckles scan.
Dynamic 30 minutes abdominal images shows focal area of abnormal tracer accumulation in peri-umblical region favoring meckels diverticulum
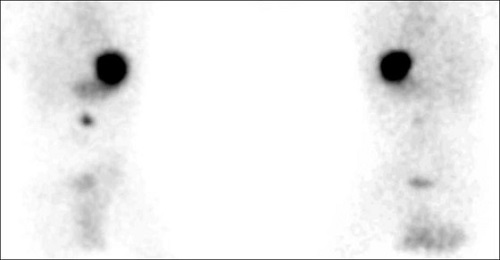
Figure 3-Thirty minutes static images shows focal area of abnormal tracer accumulation in peri-umblical region favoring meckels diverticulum.