


CASES OF THE WEEK – “A case of polystotic pagets with dorsal vertebral tubercular spondylodiscitis on whole body spect-ct skeletal scintigraphy” by Dr ShekharShikare, Consultant & HOD, Nuclear Medicine
A CASE OF POLYSTOTIC PAGETS WITH DORSAL VERTEBRAL TUBERCULAR SPONDYLODISCITIS ON WHOLE BODY SPECT-CT SKELETAL SCINTIGRAPHY
“Tuberculous spondylodiscitis (TS)”/“spinal tuberculosis (ST)” and “Pott’s disease” are synonyms which refer to the infection of the vertebral bones by Mycobacterium tuberculosis. Musculoskeletal TB accounts for approximately 10% of extrapulmonary TB cases and 1–5% of all TB cases. ST is the most common form of skeletal TB and is endemic in most of the developing countries. It is still an ongoing cause of mortality and morbidity in the twenty-first century despite advances in diagnostic methods and treatment. Because delayed diagnosis and treatment due to its indolent course result in permanent sequelae such as deformities and neurological deficits, prompt diagnosis is required to start appropriate therapy on time to prevent permanent sequelae development. Therefore, a high index of suspicion of ST based on epidemiological, past medical and/or contact history, clinical clues, and characteristic imaging findings is of paramount importance in earlier diagnosis.
Eur Spine J (1999) 8 :205–209, Shikare S et all- Bone scintigraphy in tuberculous spondylodiscitis)
Analysis- The Bone scans were analyzed and the following points were taken into consideration: 1. Skeletal areas of abnormal uptake 2. Types of uptake in the affected skeleton 3. Extra vertebral sites of skeletal affection Anti-tuberculous chemotherapy were the cornerstone of treatment for these patients. Complete neurological deficit at the time of presentation, worsening of the neurological deficit while on chemotherapy (as judged by Frankel’s grading) or persistent painful instability were used as indications for surgical intervention. Results of scintigraphy The uptake was increased in 38 out of 40 patients, while it was normal in remaining two patients, giving a sensitivity of 95%. The abnormal uptake was either of homogeneous or heterogeneous nature. Four different types of uptake were noted. Type I pattern: diffuse with disc space obliteration. Type II pattern: diffuse with central cold spot.
Type III pattern showing segmental pattern (type III) Type III: Segmental The increase in uptake in the type III pattern was patchy in the affected vertebra, with intervening areas of normal uptake. It was noted in six patients, affecting ten vertebrae (Fig. 3). Type IV: Normal Two of the patients with affection of lumbosacral junction had normal uptake, although the pathology was obvious on radiographs as well as at the time of surgery. Multicentricity was picked up in ten patients (25%). Rib lesions were noticed in six patients, affecting ten ribs. The lesion was always a diffuse band of increased uptake of varying length. No skull lesion was noted in any of the patients. Six patients had vertebral skip lesions, two of which also had a rib affection. Four different types of radiographic presentation were noted on radiological examination of the affected skeleton. 1. Paradisical affection with disc space narrowing 2. Vertebra plana 3. Anterior scalloping 4. Normal. Correlation between different types of radiographs and the scintigraphy patterns. In six patients with vertebral skip lesions, radiographs failed to demonstrate any abnormality at the site of skip lesion. The radiographs failed to show any abnormality in 12 patients (30%). In this subgroup, the scan showed increased uptake of segmental pattern in four patients, while in the remaining eight the uptake was of diffuse nature with disc space obliteration. Histopathology The diagnosis was confirmed by microbiology and histopathology of the sample collected at the time of biopsy.
Widespread availability and relative ease of performing whole-body skeletal survey make bone scan a better tool in the initial evaluation of the patient. Imaging of the entire body helps to pick up clinically silent skeletal lesions, which need not be vertebral. Identification of skip lesions can change the management protocol to a great extent in such patients. Bone scan not only helps in picking up multicentricity, but also describes the spatial extent of the lesion at the affected site. Although non-specific, this non-invasive investigation can help to narrow the differential diagnosis in a patient with vague clinical presentation. Presence of a typical rib lesion with absence of a skull lesion can be used as a supplementary evidence in suspicious cases.
In Paget's disease, the bone scan allows visualization of the whole skeleton, permitting accurate assessment of disease extent. The scan appearances are usually characteristic, and as uptake of tracer depends upon skeletal metabolic activity and reflects the severity of Paget's disease, in addition to providing early appreciation of alterations in disease activity. While correlation of x-rays and bone scans in Paget's disease have shown that neither method alone detects all lesions, it is clear that the bone scan is the more sensitive technique. In addition, those sites that are occasionally missed by bone scan are metabolically inactive. The bone scan is the investigation of choice in Paget's disease, and radiology should be used to provide supplementary information, as and when required.
Case
65 years old gentleman with history of severe dorsal spine pain for two months. MRI spine- Suspicion of D8-D9 infective spondylodiscitis with canal stenosis.
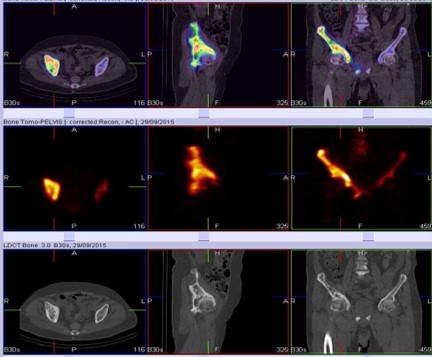
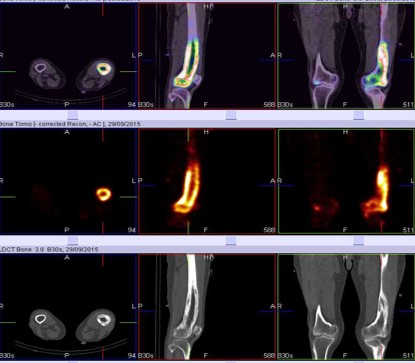
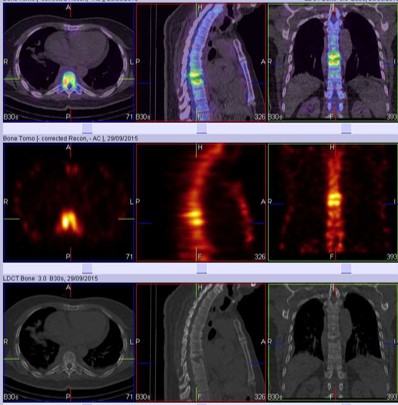
WHOLE BODY BONE SCAN & SPECT CT fused images Abnormally increased uptakes involving D8 & D9 vertebra with destruction of disc space? Infective. Abnormally increased tracer uptakes in right hemi pelvis and lower half of left femur favor polyostotic Paget disease.
Biopsy- Dorsal vertebral region-Tubercular.
Case 1
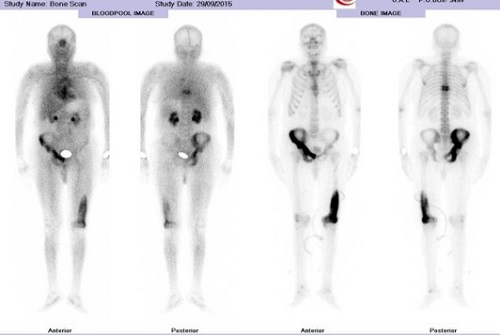
WHOLE BODY BONE & SPECT CT FUSED IMAGES
Abnormally increased tracer uptakes in right hemi pelvis and lower half of left femur favors polyostotic Paget's
WHOLE BODY BONE & SPECT CT FUSED IMAGES
Abnormally increased tracer uptakes involving D8 & D9 vertebra with destruction of disc space ? Infective.



Case 2
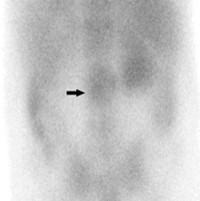
Localization of gallium uptake with SPECT/CT in a patient suspected to have a spine infection.
(a) Planar and SPECT image shows findings indicative of a spine infection (arrow). However, the location of the infection is not clear. (b–Fusion SPECT-CT images show clear correspondence between the abnormal scintigraphy findings and the defects seen at CT (arrow in d). The diagnosis of discitis with associated bone involvement was made by using both modalities.