


CASE OF THE WEEK – “Fibrous Dysplasia in Maxillary Bone: Case Report” by Dr ShekharShikare, HOD & Consultant, Nuclear Medicine, NMC Royal Hospital Sharjah
Fibrous Dysplasia in Maxillary Bone: Case Report
The incremental value of RADIONUCLIDE BONE SCINTIGRAPHY in fibrous dysplasia of bone
Fibrous Dysplasia (FD) is described as a slowly evolving, benign tumor disorder of bone development characterized by the replacement of normal bone by excessive proliferation of cellular fibrous connective tissue interspersed with irregular bone trabeculae. In 1891, Von Recklinghausen denominated de "generalist fibrous osteitis" pathological conditions that characterized deformities and bone alterations. Therefore, only in 1938, Liechtenstein and Jaffe recognized these conditions described, previously, as a well-characterized disease and named it fibrous dysplasia.
The etiology of this entity is still unknown. Clinically it is classified as monostotic or polyostotic, the first being focal, limited to a single bone, and the second, multifocal, involving several bones simultaneously.
The monostotic form shows no predilection for sex and is found in about 70% of all cases of fibrous dysplasia, with gnathic bones being the most affected sites. The cases of monostotic fibrous dysplasia are usually diagnosed during the second decade of life, with painless swelling being the most common feature.
Polyostotic fibrous dysplasia is an uncommon condition, presenting a higher prevalence for females. The number of bones affected ranges from a few up to 75% of the entire skeleton and almost all patients with polyostotic fibrous dysplasia present craniofacial involvement with surprising predilection on one side of the body. The involvement of two or more bones associated with brown-to-white pigmentation characterizes Jaffe-Lichtenstein Syndrome.
It can be evaluated by conventional radiography, scintigraphy, magnetic resonance imaging and Computed Tomography Scans (CT) although CT is considered the exam of choice in the evaluation of craniofacial lesions.
It's classified according to the number of bones affected and the presence or not of extra-skeletal abnormalities. The monostotic form affects only one bone and corresponds to 70-80% of FD cases. The polyostotic form, in which multiple bones are affected, can be divided in three subtypes: Craniofacial, in which only bones of the craniofacial are involved including the mandible and maxilla; Lichtenstein-Jaffe, in which besides the involvement of multiple bones of the skeleton are brown-to-brown pigmentations in the skin; Albright syndrome, characterized by the involvement of several bones, brown-to-brown pigmentation on the skin and endocrine impairment, with prominence for early puberty in girls. The polyostotic form responds for 20-30% of the cases.
Initially the disease is asymptomatic. The signs and symptoms in FD are dependent on the location of the lesion(s) and the compressive effect on neighboring structures as the tumor progresses slowly: Asymmetry and facial deformity; Pathological fractures; Obstruction of the paranasal sinuses generating recurrent infections, cysts and mucoceles; Anosmia, headache, loss of visual acuity by compression of the optic nerve; Alteration of ocular movements, ptosis, exophthalmos, strabismus; Conductive hearing loss.
References
Case
A 41-year-old gentleman patient with the chief complaint of painless swelling on the right side of face since three years which has started with a pea size but gradually increased. There was no history of trauma, paresthesia, and difficulty in chewing food, and it was not associated with any other symptoms. Based on clinical examination a provisional diagnosis of fibro-osseous lesion of left maxillary region was made.

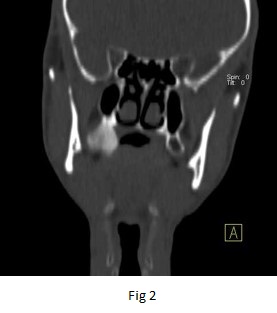
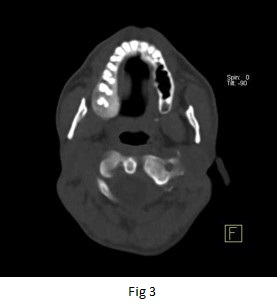
Figure 1,2,3 - CT Scan images of the face
CT scan images of the face – There is a focal expansion of the posterior-inferior aspect of the right maxillary bone involving the origin of the last three teeth. The bone shows a ground glass pattern with no cortical destruction or soft tissue component. These features favor fibrous dysplasia (figure 1,2 & 3).
Referred for 99mTc MDP whole body bone and SPECT CT scintigraphy to evaluate if it is MONOSTOTIC or POLYSTOTIC fibrous dysplasia.
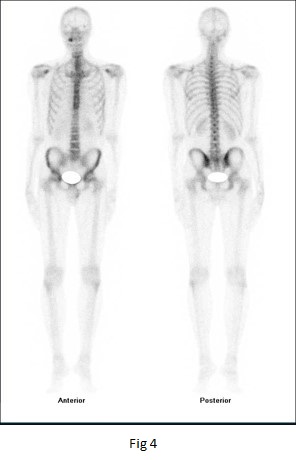
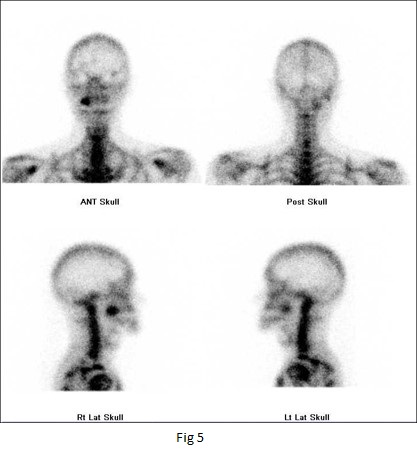
Figure 4 & 5 - 99mTc MDP whole body bone and spot images of the face.
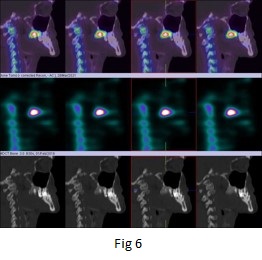
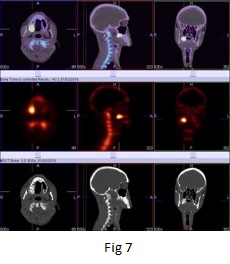
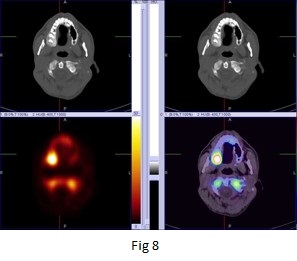
Figure 6,7 & 8 - 99mTc MDP bone SPECT CT fused images of the face.
99mTc- MDP WHOLE BODY BONE AND SPECT-CT FUSED IMAGES OF THE FACE confirms that involvement is confined to the postero-inferior aspect of the right maxillary bone, without evidence of disseminated disease. There is intense focal area of increased tracer uptakes in right maxillary bone.(figure 4 to 8).
Discussion
FD is commonly a benign lesion in which irregularly distributed spicules of bone lie in cellular fibrous stroma. The lesion is believed to be hamartomata’s developmental abnormality of bone. FD is essentially a disease of young population with incidence of 1:4000 to 1:10,000. Bones of face and skull are frequently involved, resulting in asymmetry and spontaneous fractures. Craniofacial structures are involved in 10% of monostotic type, 50% of mild polyostotic cases, and 100% of severe polyostotic cases. Maxilla and mandible are commonly affected with the temporal bone involved in 18% of cases.
CT scan face images shows focal expansion of the posterior-inferior aspect of the right maxillary bone involving the origin of the last three teeth. The bone shows a ground glass pattern with no cortical destruction or soft tissue component.
Radionuclide bone scans are of certain value in the diagnosis of FD and useful in determining the extent of the skeletal involvement especially in polyostotic lesions. The diagnostic specificity of FD with radionuclide bone scanning can be improved in association with other imaging modalities such as X-rays. CT scan with contrast, SPECT-CT enhances sensitivity for lesions detection over planar bone scintigraphy. In addition to improve anatomic localization of scintigraphy findings, this equipment offers the opportunity to add true diagnostic information derived from CT imaging.
Literature stated the diagnosis is generally clear after a proper radiological and scintigraphy workup. However, biopsy might be needed if the diagnosis is doubtful or malignant transformation is suspected.