


CASE OF THE WEEK – “A rare case of Imperforate Anus Surgery performed in 36 hours old baby weighing 1.6 kg” by Dr. Wissam Altamr, Specialist, Paediatric Surgery at NMC Royal Hospital, Sharjah
A rare case of Imperforate Anus Surgery performed in 36 hours old baby weighing 1.6 kg by Dr. Wissam Altamr, Specialist Paediatric Surgeon.
A pre-term baby boy (32 weeks gestation by LMP) had a rare anomaly imperforate anus (absence of anal opening) and a big right inguinal hernia. The baby was delivered by emergency CS due to scar tenderness. The baby developed grunting and tachypnea and was shifted to NICU under the care of Dr. Jayasheela Kannan, Specialist Neonatologist.
In NICU, CPAP started to assist for troubled breathing. Dr Wissam Altamr (Pediatric Surgeon) examined the baby and explained to the father about the baby’s rare condition. After discussion with the father, Dr Jayasheela, and Dr Ayman Moustafa, Consultant Anaesthesiologist.
The decision was to treat the baby in our hospital and to perform the surgery after preparing the baby and exclude another anomaly. IV fluids, IV Antibiotics and IV Caffeine started for the baby and septic work-up was done.
The baby also underwent cardiac echo & consultation was done by Dr Al Kamali, Consultant Paediatric Cardiologist. The diagnosis revealed a small PDA and a cranium ultrasound was performed which was normal.
A USG Abdomen performed showed bilateral pelvi-calyceal system fullness. When the baby was of 24 hours of birth, prone cross table lateral radiograph was done. Dilated rectum and the distance measuring >1 cm from the anal marker.
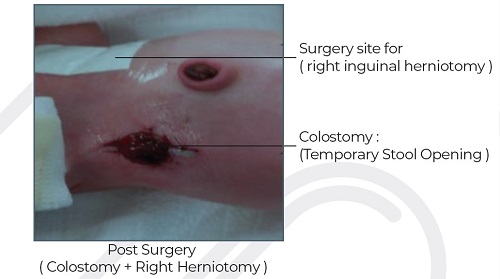
At 36 hours of birth and when the baby was weighing 1.6 kg, the Emergency Colostomy and right Herniotomy surgery was performed by Dr Wissam Altamr. The patient tolerated the procedure, was extubated and shifted to NICU.
24 hours after the surgery, the baby received initial OGT feeds which was then increased gradually to full feeds. The baby is doing well and the colostomy is working perfectly. After the surgery, the baby passed meconium through colostomy. The baby gradually started to gain weight, then 14 days after birth, he was advised for discharge in good condition.
Dr, Wissam explained to the parents the future treatment plan for the baby that he needs 2 more surgeries. The Paediatric Surgery Department in NMC Royal Hospital, Sharjah is preparing for the Anorectoplasty surgery at 5 months of age.


Before surgery - Imperforate Anus (Absence of anal opening)
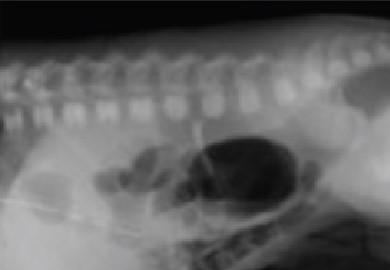
Prone cross table lateral radiograph of a neonate at 24 hours of age demonstrating a dilated rectum (arrow) measuring >1 cm from the anal marker
What is imperforate anus (Anorectal Malformations )?
Imperforate anus occurs when the anal opening is absent or not in a normal position. It is a birth defect caused by the failure of normal development of the anal area. Sometimes an abnormal opening (fistula) is present between the bowel and the vagina in girls, or between the bowel and the urinary tract in boys.
What causes an imperforate anus?
There is no known cause for the condition, which occurs in 1 out of every 5,000 infants. They are slightly more common in males. Sometimes imperforate anus occurs as a part of a syndrome. These syndromes include other developmental issues. They can include: VACTERL syndrome, CHARGE syndrome, Currarino syndrome or Townes-Brocks syndrome.
Some of these syndromes are linked to problems with certain genes. Many genes may play a role in causing imperforate anus. Environmental factors may also play a role in this condition. These include exposure to alcohol, substances, or some infections. It isn’t clear which factors raise the risk for this problem.
What are the symptoms?
No anal opening • misplaced anal opening • anal opening very near the vaginal opening in a female • no bowel movement within 24 to 48 hours after birth • stool passed through the vagina or urethra • abdominal distension.
How is it diagnosed?
Diagnosis is made at birth when the anal opening is checked during the newborn’s physical examination.
Types of ARMs (Imperforate Anus)
Each type of ARM has unique characteristics. ARM affects each child differently. Whether a child has any problems depends a great deal on the type of ARM the child has:
Below are the most common types of ARMs in children.
Boys:
ARM with recto-perineal fistula.
ARM with recto-bulbar fistula.
ARM with recto-prostatic fistula.
ARM with recto-bladder neck fistula.
ARM without fistula.
Girls:
ARM with recto-perineal fistula.
ARM with recto-vestibular fistula.
ARM with recto-vaginal fistula.
ARM without fistula.
Cloaca.
What is the treatment?
Each child with an anorectal malformation has unique needs. The care team will create a treatment plan based on your child’s type of ARM, the presence and type of associated conditions, and overall health. Working together, these experts can help your child have the best quality of life possible.
Posterior Sagittal Anorectoplasty (PSARP)
Children who have an ARM will need a surgery called a PSARP to correct the defect. This procedure is often called an anorectoplasty. It involves moving the anus to the location within the muscles (anal sphincter) that control the bowels. This surgery allows gas and solid waste to leave the body. It may occur soon after birth or later. Timing depends on the child’s needs.
Colostomy Surgery
Prior to the PSARP, some children have a colostomy. This surgical procedure involves creating an opening (stoma) in the abdominal wall and bringing a segment of the large intestine out through the opening. This creates a way for solid waste and gas to pass through the body until the PSARP can take place. The surgeon also creates a second opening called a mucous fistula. This helps the team perform diagnostic testing prior to the PSARP. The surgeon will close the colostomy a few months after the PSARP, since it will no longer be needed.