


Sleep-Disordered Breathing


What is sleep-disordered breathing?
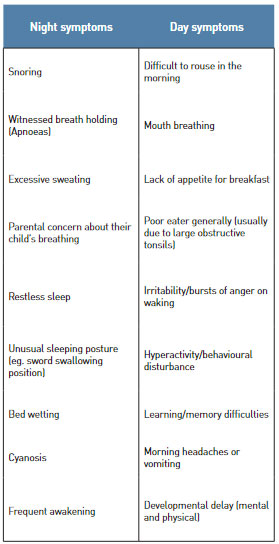
Sleep-disordered breathing covers a variety of conditions ranging from snoring to absence of air flow to the lungs because of obstruction in the nose and/or throat (physical obstruction). Mild snoring is not a medical problem; most children will snore at some stage of their lives. However, severe snoring is not only a social problem but may be associated with frequent events of partial or complete upper airway obstruction during sleep. Approximately 25% of all children (one in four) are affected by sleep disordered breathing. Sleep-disordered breathing occurs mainly between the ages of 2 and 8 years. Earlier onset is associated with children who have head, face or nervous system problems; later onset is linked to obesity.
How is sleep-disordered breathing diagnosed?

The diagnosis is made on taking a detailed history, with particular reference to the symptoms mentioned in the Table. Clinical examination, lateral neck x-ray (to assess the size of the adenoid) and overnight sleep study (continuous pulse oximetry) are helpful in confirming the diagnosis.
Lateral neck x-ray showing enlarged adenoid obstructing the upper airway.
However, the gold standard investigation is a complex sleep study called polysomnography but it is expensive and therefore reserved for abnormal children or special cases only.
Why is sleep-disordered breathing a big problem?
Children with sleep-related breathing disorder experience reduced health status, retarded growth and development as well as poorer quality of life. The presence of obstructive sleep apnoea also increases the chances of heart and lung-related complications. Treatment of the condition can prevent these negative consequences.
How is sleep-disordered breathing treated?
In normal children, medicines for nasal blockage sometimes are helpful, but in most cases the cure is to remove the adenoid and tonsils. In children with craniofacial deformities complex upper and lower jaw repositioning surgery may be needed.
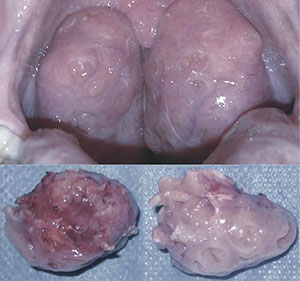
Large obstructive (kissing) tonsils at the back of the throat and surgical specimens of tonsils
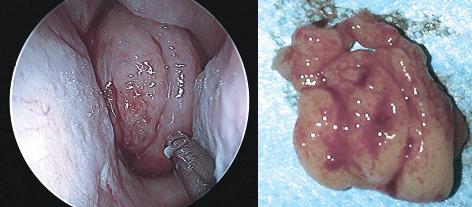
Large obstructive adenoid at the back of the nose and surgical specimen of adenoid (looks like a bunch of bananas)